
Innovating Through Irritation with Dr. Jordan Shlain
Shlain presented as part of a speaker series for the Caltech Longevity Club, which is led by Andrea Olsen (CNS/BEM ‘27). Other club leaders include William Wang (BS ‘29) as Vice President and Team Members Mahi Ravi (ChemE ‘26, Lloyd) and João Pedro Bra Cardoso Ferreira Bastos (CS ‘26, Blacker). (Photo: Caltech Longevity Club)
Dr. Jordan Shlain, who presented to the Caltech Longevity Club on January 28, framed his work as a form of moral friction: a refusal, throughout his career, to accept incentives that reward sickness over health. A physician-entrepreneur and civic leader in San Francisco, Shlain has built his companies and philosophy around a single organizing principle: trust.
Shlain is the founder of Private Medical, a concierge-style primary care practice built on a “trust-first” model of personalized, preventive medicine. He previously founded HealthLoop, an early clinical engagement and workflow automation platform designed to track patients between visits and reduce post-discharge complications and hospital readmissions. Beyond medicine, he has worked to improve school nutrition through Eat Real, served in governance roles on San Francisco boards and commissions (including the Health Services Board and Entertainment Commission), and acted as Editor-in-Chief of Tincture, a digital publication covering health, science, technology, and policy.
His organizing principle is simple: if you want better outcomes, fix incentives — and start upstream.
Shlain’s critique begins with a structural shift in American healthcare. Decades ago, health insurance functioned like other forms of insurance: a hedge against catastrophic events. But as insurers evolved into “health plans,” primary care became the intake valve for a system that profits from complexity: surgeries, high-cost drugs, procedures, hospital readmissions.
The result? A primary care physician managing 3,500 to 5,000 patients, seeing thirty a day, with minutes per visit. “You can get through maybe a single issue,” Shlain explained in an interview with the Tech. “How can anybody manage that many people with any degree of consistency or quality?”
Concierge or direct primary care, in his view, attempts to reconstitute the doctor-patient relationship. Patients pay directly for a physician with a dramatically smaller panel. That time buys more than longer appointments: it buys context — family history, stressors, goals, preferences — and post-visit work (research, specialist calls, follow-ups) that traditional billing structures don’t reimburse.
The question shifts from “What’s the matter with you?” to “What matters to you?”
Shlain contends that this model improves population health within its cohort, lowers burnout among physicians, and — if practiced well — reduces total system costs by preventing downstream crises. The irony, he suggests, is that a system built to monetize transactions has little appetite for fewer transactions.
Trust as operating system
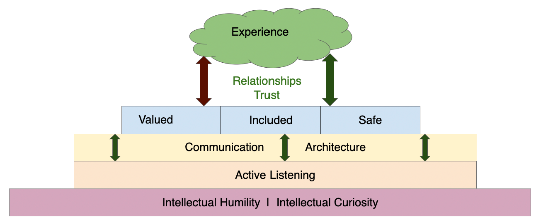
The multiple levels of communication and trust architecture that define Shlain’s business practices. (Image: Jordan Shlain)
Trust, operationally, requires eliminating supply-side moral hazard. At Private Medical, physicians do not profit from ordering tests, prescribing medications, or referring to specialists. Revenue is fixed annually. If patients get sicker, the workload rises without financial gain. Outcomes and incentives are on the same ledger.
Trust also emerges from culture. Hiring prioritizes what Shlain calls “natural healers,” or doctors drawn to medicine as a calling. Retention rates exceed 95% over two decades. Communication is architecturally encoded: phone, text, and email are available, but used within an implicit social contract. A 2 a.m. call signals urgency, not anxiety. Over time, doctor and patient develop rhythm and mutual respect.
“The 24/7 promise,” he clarified, “is really about trust, not availability.” Burnout, he argues, stems less from being needed than from being reduced to a billing code processor.
Prevention without the circus
Prevention, in Shlain’s framework, is strategic rather than performative. Foundational interventions such as sleep, exercise, diet, fiber intake, blood pressure, and lipid control remain the highest signal-to-noise moves for most healthy adults. (He quipped that fiber deserves more hype than protein; gut-produced short-chain fatty acids influence satiety and serotonin production.)
Risk assessment proceeds in layers: foundational metrics, then genetics and advanced imaging, then highly targeted intervention. Daily lifestyle strategy, not without replacing judgement.
Shlain is sharply critical of what he calls the “longevity circus”: unvalidated peptides, wellness IV drips (with potentially nonapproved contaminant levels), aggressive biomarkers, and biohacker maximalism. “Longevity is not a biomarker-deficiency syndrome,” he said. Quarterly lab panels often amplify false positives without improving outcomes.
More is not better. “Better is better.”
The key statistical concept is pretest probability. When the likelihood of disease is low and the false positive rate exceeds that baseline risk, testing can generate cascades of unnecessary interventions — what Shlain deems “medical theater.” He quantified risk: instead of evidence, risks becoming a “lottery system for false reassurance.”
His counsel: don’t refuse access to data with expertise. Tacit knowledge, earned through training and pattern recognition, cannot be crowdsourced from search engines or alone.
HealthLoop and the incentive problem
At HealthLoop, Shlain sought to improve post-operative follow-up and clinical communication. The platform reduced hospital readmissions — by as much as 50% in certain contexts — via structuring check-ins and surfacing early warning signs.
But success collided with perverse incentives. Hospitals are reimbursed more for readmissions. Lowering complications, in a free-for-service paradigm, erodes revenue.
Healthcare innovation, he argued, repeatedly “goes to die” at the payment layer. Federalism compounds that challenge: healthcare is not one national system, but fifty regulatory regimes. Add a workforce shortage in primary care and your can’t software your way out of a people problem.
Two-Tier critique — and a rebuttal
Concierge medicine is often criticized as entrenching a two-tier system. Shlain’s steelman from our interview acknowledges the optics: if some can “power up” their care, inequities may widen.
His counterargument is comparative. Education, housing, transportation, and food already operate in tiered markets with baseline public access and optional private augmentation. Why, he asks, is healthcare uniquely expected to resist this structure? Provided a strong baseline exists for all, innovation at the high end can fund experimentation and eventually democratize improvements — much like early electric vehicles that began at luxury price points before scaling.
Still, he emphasizes support for AI and other tools to broaden access. The ethical guardrail, in his view, is whether better care for some comes at the expense of others.
AI: amplifier or eraser?
Shlain remains optimistic about AI, but wary.
The risk is not that AI will replace physicians outright; it is that institutions will use AI to automate the relationship out of medicine. Insurers could deny claims faster. Pricing could grow more opaque. Information asymmetry could intensify, Shlain warned.
In response, Shlain has proposed a “Hippocratic Oath for the AI era”: a requirement that algorithms and institutions demonstrate, transparently and continuously, that they do no harm. The departures from Hippocrates are twofold: AI binds not only individuals, but also institutions, and it explicitly addresses the exploitation of patient data — which he describes as “an extension of the patient’s body and dignity,” such that treating it as a commodity constitutes a violation.
The technology exists to audit outcomes in real time. Whether the will exists to demand accountability remains open.
And if you want to live well, don’t spend your life chasing biomarkers. Spend it doing what you’re great at.
Irritation as innovation
The talk’s title was less a slogan than a posture. It is the refusal to accept burnout as inevitable, to accept incentives misaligned with health, to accept that more data equals more wisdom. It is irritation with a system that monetizes sickness — and belief that trust, properly engineered, can be scalable.
At Caltech, where STEM culture prizes first principles, Shlain’s message resonated as both structural critique and ethical invitation: if you redesign the incentives, the behavior follows. If you restore the relationship, prevention becomes possible.
In closing — book recs!
Jordan Shlain closed his talk with a plethora of book recommendations. These were:
- Humility Is the New Smart by Edward D. Hess & Katherine Ludwig
- The Secret Life of Pronouns by James W. Pennebaker
- Social: Why Our Brains Are Wired to Connect by Matthew D. Lieberman
- Ignorance: How It Drives Science by Stuart Firestein
- The Truth About Trust by David DeSteno
- Palaces for the People by Eric Klinenberg
Together, they mirror the themes of Shlain’s talk: humility, language, social connection, uncertainty, trust, and the civic infrastructure that makes human flourishing possible.
Thank you, Dr. Shlain, for taking the time both to present on our campus and have a follow-up conversation for our newspaper. We appreciate it tremendously.
Caltech Longevity Club members with Dr. Jordan Shlain. Left to right: JP Bastos, Shlain, Andrea Olsen, and Ayush Natarajan. (Photo: Caltech Longevity Club)